


Part one of two. Part two walks through CPOW-SAD letter by letter.
Transport gets most of the attention: the packing, the battery math, the oxygen tank, the elevator, the door frames, the trip there and the trip back. And it should. Moving an ECMO patient is one of the riskiest things we do.
But I have learned to respect the moment right after transport just as much.
Back in the ICU room. Back from CT. Back from the OR. The patient is settled. The team is busy. Everyone exhales a little. That exhale is the problem. The first five minutes after a move may be the easiest time to miss a preventable error, because everything looks like it is back where it belongs.
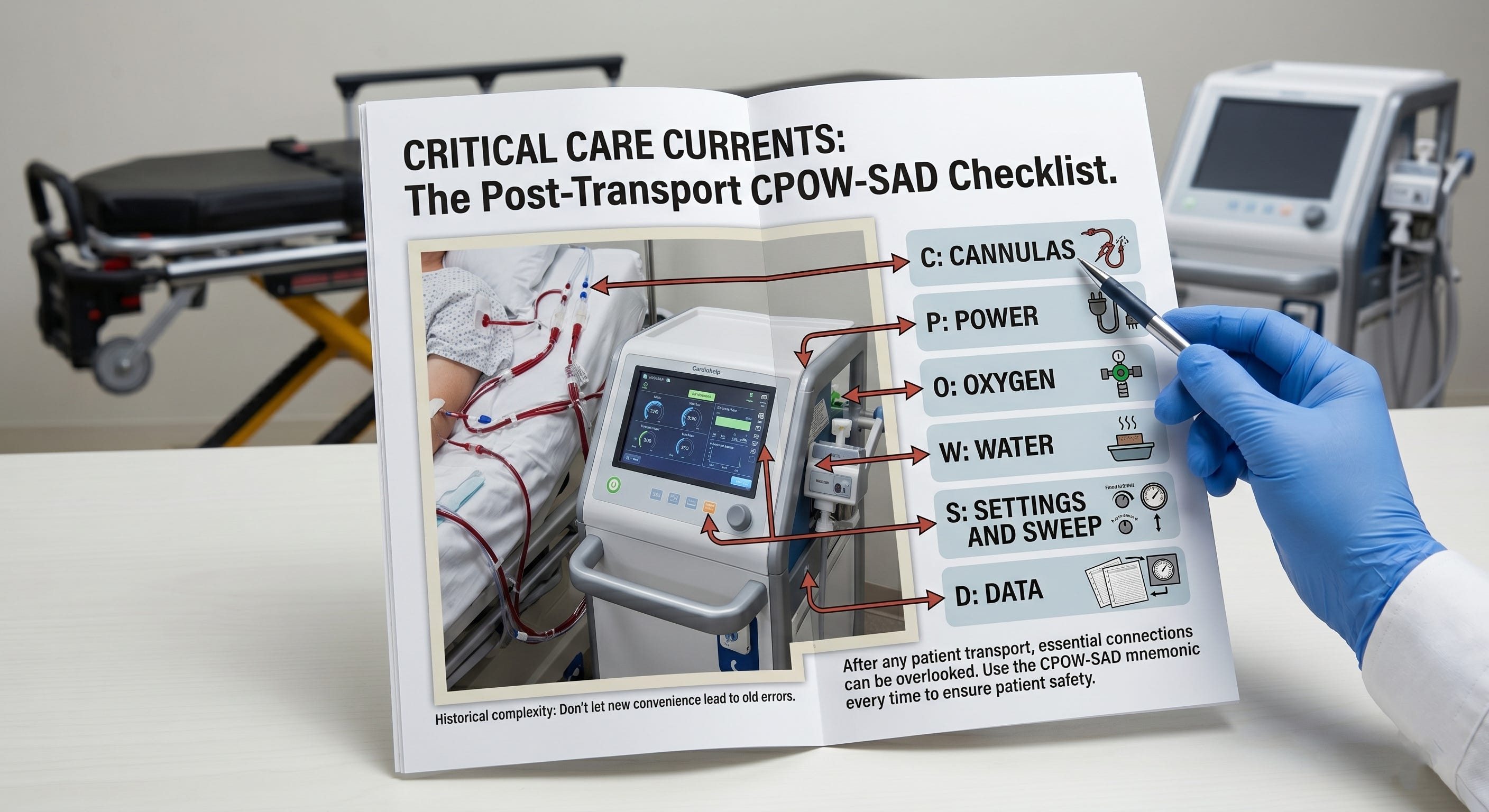
So I run a reset every time. The mnemonic I use is CPOW-SAD:
C - Cannula
P - Power
O - Oxygen
W - Water
S - Sweep and settings
A - Alarms
D - Data
That sequence is not random. Secure the patient. Restore the supplies the machine depends on. Confirm the machine is running at the right settings. Arm the safety net. Make sure the data is transmitting. Part two will walk through each letter in detail. This first part is about the idea underneath the mnemonic.
The main idea: connected is not the same as working
If you remember one thing, remember this: connected is not the same as working.
After a move, the danger is not always that something is missing. Often, the danger is that something is present but not doing its job. The power cable may be in the wall, but not seated in the machine. The gas tubing may be connected, but the flowmeter may still read zero. The heater-cooler lines may be hooked up, but the unit may still be cold. The cannula may still be sutured, but it may have shifted during the slide from bed to table, or table to bed.
Everything looks attached. The console looks calm. That is the trap.
CPOW-SAD is not a “did I plug it in?” list. It is an “is it actually functioning?” list. Every letter asks the harder question. Not just, “Is it there?” but “Is it secure? Is it powered? Is gas actually flowing? Is water warm and circulating? Are the settings back where they should be? Are the alarms armed? Is the data transmitting?”
Why this matters after transport
There is a reason this happens after transport. The team is task-saturated. Everyone is trying to get the patient settled. Sources are being switched from portable to wall. Cables are being moved. Tubing is being reorganized. The patient has just been moved from one surface to another, and anything taped, sutured, clipped, connected, or positioned can shift.
That combination matters: high workload, physical movement, source changes, a quiet console, and a team that thinks the hard part is over.
That is exactly when a reset helps. A pump can be spinning at full flow with the gas off. A cable can sit in the wall and charge nothing. A circuit can look perfect while two centimeters of cannula migration changes everything. So I do not trust the calm console. I walk it.
Do not leave the room SAD
There is a hook inside the hook. The front part is familiar: CPOW. Cannula. Power. Oxygen. Water. Those are the visible things. They are easier to remember because they feel physical.
But the back half matters just as much: SAD. Settings. Alarms. Data.
Those are the ones I see skipped most often, because they are less visible. Nothing falls on the floor when you forget them. The patient may simply drift in the wrong direction, unwatched or undocumented. That is why the tail does its own work: do not leave the room SAD.
Before I leave, I want settings correct, alarms armed, and data flowing.
A shorter version like POW is easier to remember, but look at what it drops: cannula and sweep. Those are high-stakes checks. Shorter is not always safer.
Saying it out loud
When a family member is at the bedside, I will sometimes run CPOW-SAD out loud. Not dramatically. Just calmly: “I’m checking the cannula. Now power. Now oxygen. Now water. Now sweep and settings. Now alarms. Now data.”
That does three things. First, it reassures them. They see deliberate care instead of silent activity around tubing and machines. Second, it steadies me, because explaining the steps gives my own focus somewhere to go. Third, it forces honesty. You cannot say “power is on AC and charging” out loud while staring at a battery icon and not catch the problem.
The person at the bedside becomes part of the check. That is not bedside manner added at the end. It is part of the method.
The point
For me, CPOW-SAD is less about memorizing letters and more about respecting the first few minutes after a move.
That is when small misses hide in plain sight.
A cable can be present but not charging. Tubing can be attached but not flowing. A cannula can look secure but still move. So I try not to rush that moment. Connected does not mean it is working until I confirm it.
Next: Part two, CPOW-SAD letter by letter. What each check actually catches at the bedside.
Learn more
For more practical ECMO articles and study tools, look around on this website LifeSupport.Training and subscribe to this newsletter ECMO 143: AI-Assisted Journey.
I also built AI ECMO Educator, a free-to-use tool that provides evidence-based ECMO and ECPR guidance for ICU clinicians and trainees, covering physiology, cannulation, anticoagulation, circuit management, and troubleshooting. It draws from sources such as ELSO, PubMed, AmSECT, and leading centers.
Disclaimer
This content is for educational purposes only and does not replace clinical judgment, institutional protocols, or consultation with your ECMO team.