



Recently, I heard about a patient with SAM, systolic anterior motion of the mitral valve. I had never heard of it before, and even after it was explained, I still had questions. That’s been happening more often. Adult ECMO patients don’t just come with diagnoses. They come with physiology that is not always obvious at the bedside.
We often describe ECMO as a bridge to recovery, transplant, device, or decision. But that only helps if we are clear about what the patient is being bridged from. Most of the time, the real problem is not the diagnosis itself. It occurs when the body can no longer deliver oxygen to tissues safely.
When I say oxygen delivery, I do not just mean oxygen in the blood. I mean, oxygen actually reaching the organs. That depends on several things working together: the lungs have to oxygenate the blood, hemoglobin has to carry that oxygen, the heart has to move blood forward, and the circulation has to get that blood to the tissues. If any part of that system fails badly enough, the patient may start moving toward ECMO.
That shift changed how I think about ECMO. Instead of starting with disease labels, I am trying to start with a simpler question: what part of oxygen delivery has failed?
ECMO Is a Bridge, but the Failure Comes First
A patient does not go on ECMO simply because they have pneumonia, ARDS, myocarditis, pulmonary embolism, or cardiogenic shock. Many patients have those diagnoses and never need ECMO. ECMO enters the conversation when something more fundamental breaks down. Either the body can no longer maintain oxygen delivery, or the support required to maintain it is starting to cause harm.
I needed a way to organize that at the bedside. Not a protocol, just a way to think through what is actually failing.
Here is the simple framework I am using:
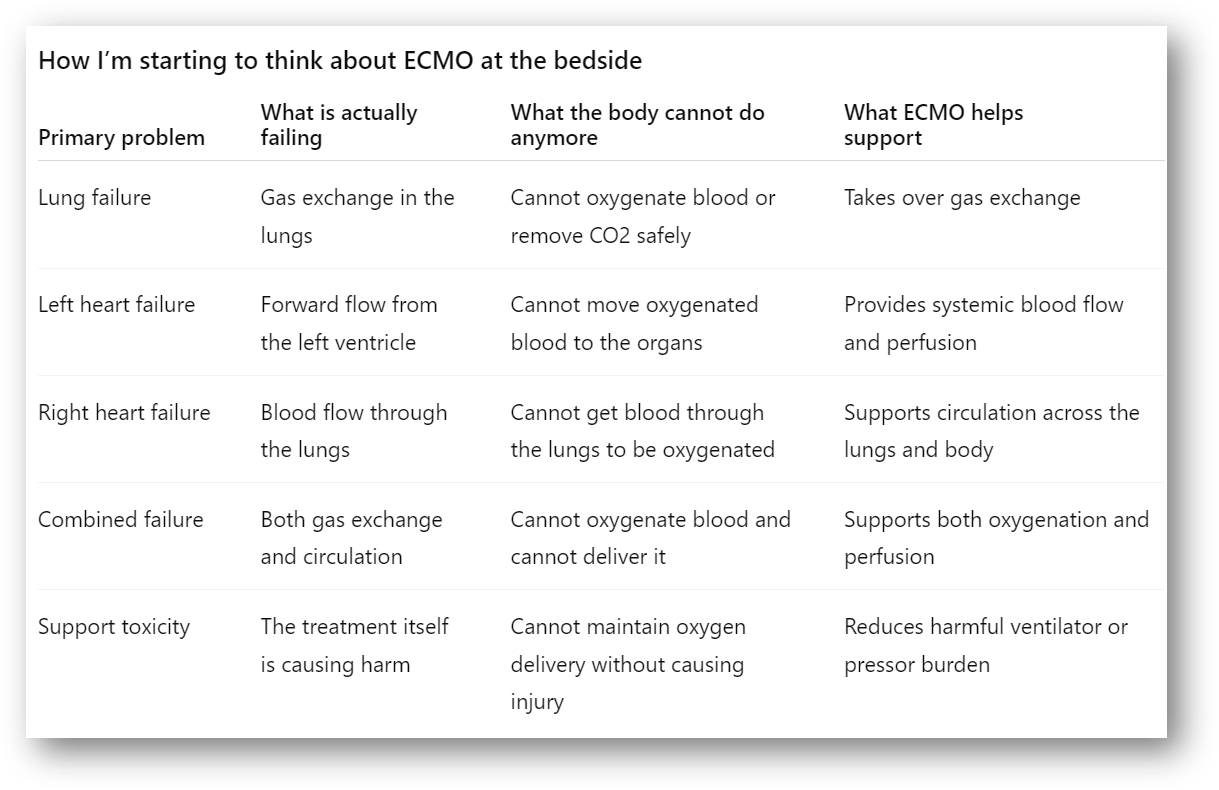
This is simplified. Real patients do not stay in clean categories, and support strategies often overlap. But it gives me a place to start.
Lung Failure: When Gas Exchange Breaks Down
In lung failure, the main problem is gas exchange. The heart may still be able to move blood forward, but the lungs cannot oxygenate the blood, remove carbon dioxide, or do either without causing further injury from the ventilator.
This is where VV ECMO usually makes sense. It takes over gas exchange while the patient’s own heart continues to provide circulation. The important question is not just whether the oxygen level is low. It is whether the lungs are the main failed system, and whether the heart can still move blood forward.
Pump Failure: When Flow Is the Problem
In pump failure, the issue is different. The blood may contain oxygen, but the heart cannot move enough of it to the tissues. Oxygen is present, but it is not getting where it needs to go.
This is what we are really dealing with in cardiogenic shock. The problem is not just a weak heart. The problem is inadequate flow and poor tissue perfusion. VA ECMO can support circulation in this setting by providing flow and pressure while the team treats the underlying cause or decides what comes next.
Sometimes the heart recovers. Sometimes it does not. The next step may be a temporary device, a durable VAD, transplant evaluation, or a difficult conversation about goals of care.
Right Heart Failure: When Blood Cannot Reach the Lungs
Not all heart failure is left-sided. In pulmonary embolism, severe pulmonary hypertension, or acute right ventricular failure, the right ventricle cannot move blood through the lungs.
If blood cannot get through the lungs, it cannot be oxygenated. It can also not fill the left side of the heart. Over time, that leads to reduced systemic perfusion. So the problem is not just “heart failure.” The problem is that blood is not making it through the pulmonary circulation.
When the Picture Is Mixed
Some patients do not fit neatly into one category. A patient with severe ARDS may also have septic cardiomyopathy. A post-arrest patient may have both lung injury and myocardial stunning. A patient on VA ECMO may develop differential hypoxia, in which the upper body receives poorly oxygenated blood from the native heart and lungs, while the lower body receives oxygenated blood from the ECMO circuit.
In these cases, the physiology is mixed. Both gas exchange and circulation may be failing. This is where hybrid strategies come into play. I try not to start with the configuration. I try to stay with the underlying problem.
If gas exchange is failing, that needs support. If circulation is failing, that needs support. Sometimes both need attention at the same time.
When Support Becomes Part of the Problem
Another piece I am paying closer attention to is the cost of conventional support. Sometimes, ECMO is considered not only because the patient is deteriorating, but because the treatments required to keep them stable are causing harm.
High ventilator pressures can worsen lung injury. Severe acidosis can destabilize the patient. Increasing vasopressor doses may maintain blood pressure while tissue perfusion continues to fail.
ECMO adds risk. It is not a neutral intervention. So it has to create a path that did not exist before. That path might be recovery, transplant, a device, an intervention, or simply time to understand whether recovery is possible.
The Question I Am Trying to Ask Better
The SAM case reminded me how much I still have to learn, but it also changed the question I want to ask. When I hear that a patient is going on ECMO, I do not only want to ask what diagnosis they have.
I want to ask what physiology failed, and what we are trying to buy time for.
That feels like a clearer way to understand ECMO as a bridge. Not just a bridge to something, but a bridge from a specific physiologic failure toward a specific possible next step.
Disclaimer
This article is for educational purposes only. It reflects my ongoing learning as an ECMO specialist and does not replace clinical judgment, institutional protocols, or guidance from your ECMO team.